World's First AI Doctor
Pioneering the future of proactive and precise healthcare by Reducing Human Error and Improving Patient Care.serious harms (deaths or permanent disability) annually Due to Diagnostic Errors in United States
Annual Deaths Due to Diagnostic Errors in India
16%
preventable harm in healthcare system
1 in 20
Adults experience a diagnostic error each year in OECD Countries
These are the numbers we aim to reduce with AI-powered innovations by directly Adding AI to EHRs.

Homo Habilis
LEARN MORE
Homo Habilis

Homo Erectus
LEARN MORE
Homo Erectus

Rudolfensis
LEARN MORE
Rudolfensis

Neanderthal
LEARN MORE
Neanderthal

Homo Sapiens
LEARN MORE
Homo Sapiens
Quick Demo of How Homo Sapieus EHR Works
Skin score
Thymus
Eos
CA 125
Vitamin B12
Serum ferritin
CTCA
Blood lead
HbA1c
Dust mite allergy
Insulin
Fat mass index
Magnesium
Neutrophils
Serum zinc
Vitamin D
Serum iron
Basophils
Gastroscopy
Cat allergy
Gamma-GT
Haematocrit
PSA
FSH
LH
Liver-fibroscan
ALP
Bilirubin
HDL
Triglycerides
Gamma-GT
Haematocrit
PSA
FSH
LH
FSH
100+
biomarkers
One clear path.
From advanced blood markers to bone density, we analyse thousands of data points to help you determine where your health is heading — and the exact steps you can take to change it.
Healthcare that connects the dots.
By analyzing your unique biomarkers, we can project a personalized timeline of your health, showing potential risks and the key moments where intervention can change your outcome.
Diabetes

Blood Sugar Increase
Month 1

Increased Thirst
Month 3

Persistent Fatigue
Month 6

Blurred Vision
Month 9

Pre-Diabetes Diagnosis
Year 1

Nerve Damage Risk
Year 2
Take Control
Early detection is the key to a better future.
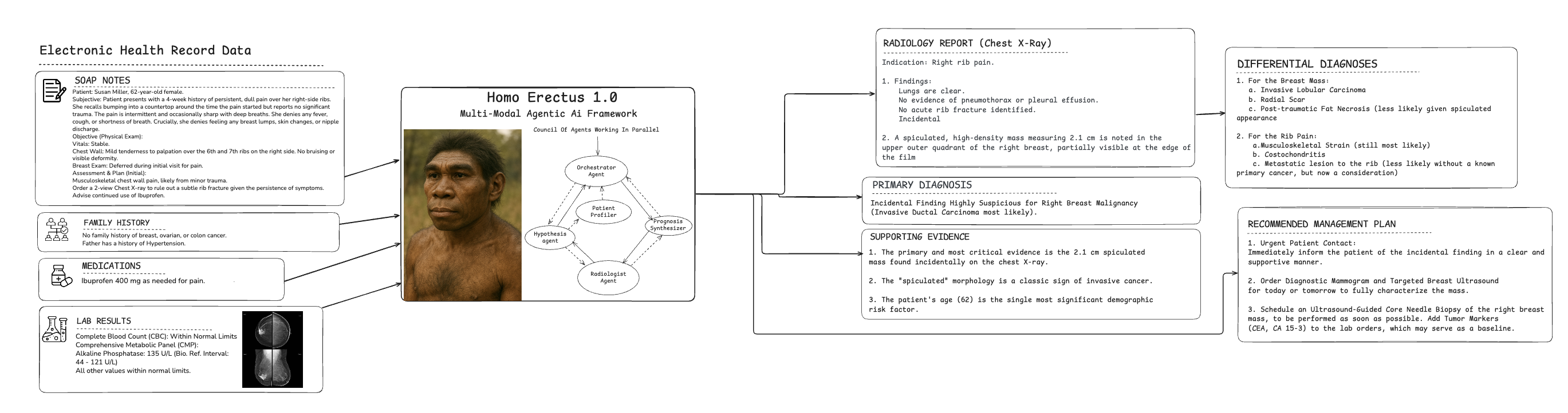
Pre-Diagnostic of Disease Using Homo Erectus (Text + Image)
Before the Breast Cancer Develops
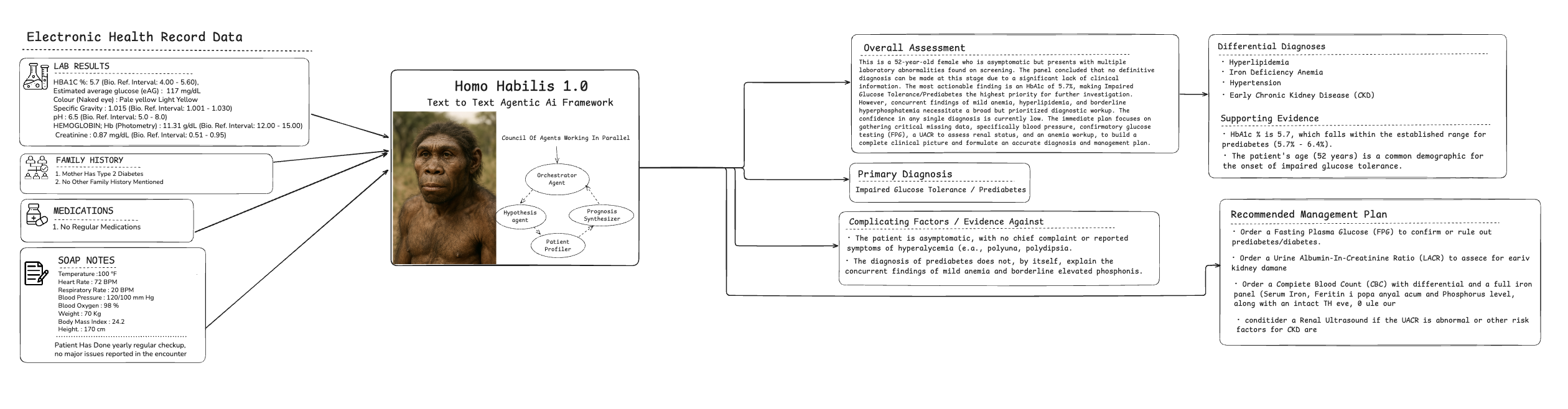
Pre-Diagnostic of Disease Using Homo Habilis (Text to Text)
Before the Diabetes Develops
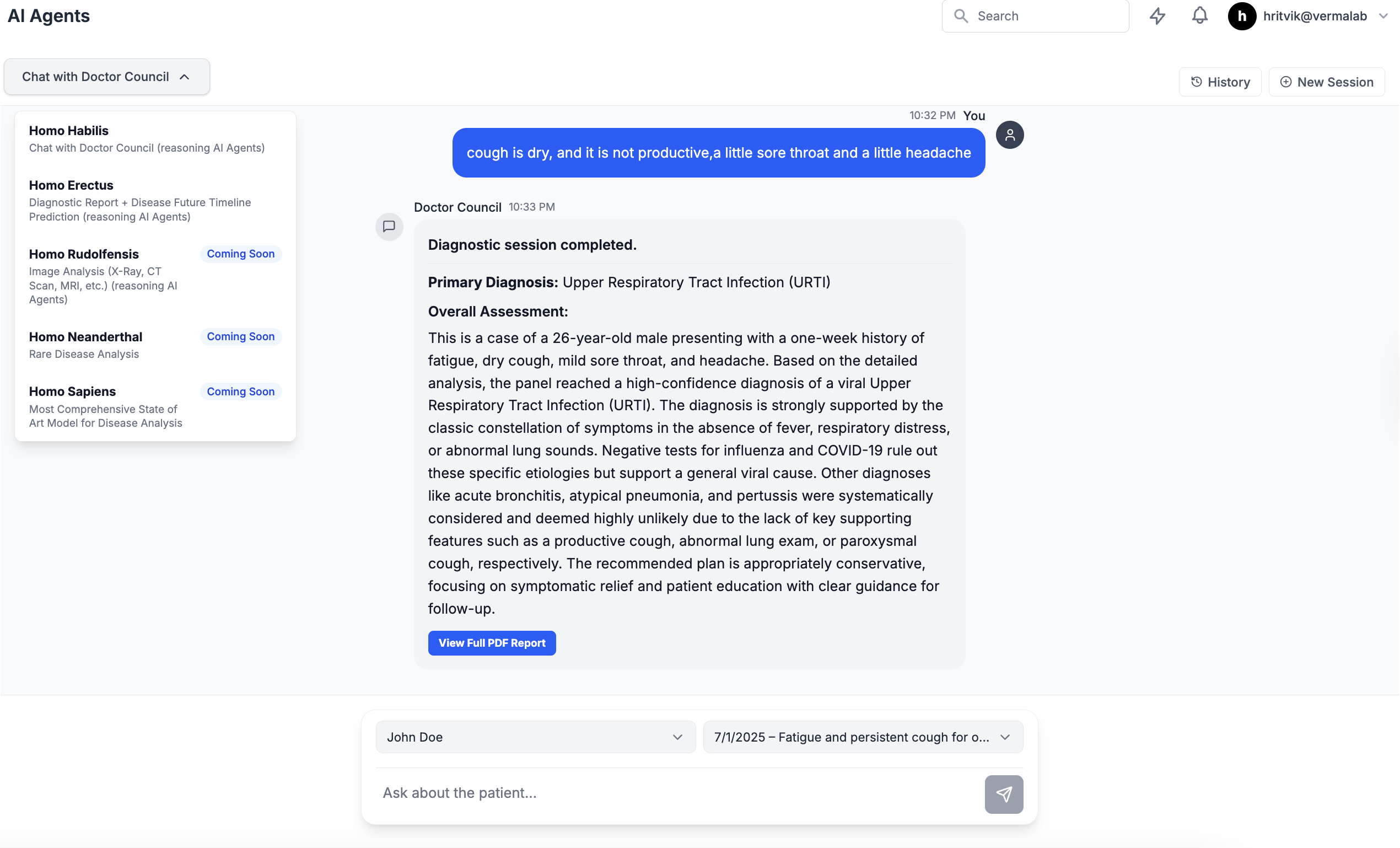
For Doctors, Use Homosapieus Council Of Doctors To Get Your Diagnosis
For Patients, Actionable Health Insights at a Glance, Powered by Your Data
Insights
Optimal
Out of range
Improving
Insufficient data
New data
All results
Cholesterol
Crucial for various bodily functions – but high levels can lead to the buildup of plaques in arteries, increasing the risk of heart disease and stroke.
Electronic Health Records Reimagined with AI Copilot
For Faster, Data-Driven Decisions
Patient Management
List Patient
Sarah Johnson
Type 2 DM | Migraine
Last visit: 09:00 AM
John Doe
Hypertension
Last visit: Yesterday
Alice Miller
Asthma | Allergic Rhinitis
Last visit: 3 days ago
Sarah Johnson
MRN: MRN8B2C7C15 • Female • 26 years
Latest Vitals (08:42 AM)
Medical History
Type 2 Diabetes Mellitus active
14 Jul 2023 • HbA1c 8.2 %
Migraine without aura episodic
2019 • 3–4 attacks / month
GERD chronic
2021 • PPI therapy
Quick Stats
18
Appointments
3
Pending Labs
2
Alerts
Upcoming Events
- Cardiology follow-up14 Aug 09:30
- HbA1c recheck22 Aug 08:00
- Ophthalmology screening05 Sep 14:15
AI-Powered Diagnostic Report
Primary Diagnosis
Acute Upper Respiratory Infection, suspected viral etiology, in T2DM patient.
Differential Diagnoses
- Pneumonia
- DKA
- HHS
- Influenza
- COVID-19
Evidence For
- The patient's presentation is consistent with an acute upper respiratory infection.
- The diagnostic plan is predicated on symptoms such as cough, fever, and other URI-associated complaints.
Evidence Against
- The presence of Type 2 Diabetes Mellitus is a significant complicating factor that argues against a simple, uncomplicated diagnosis without further investigation.
- An acute infection in a diabetic patient increases the risk for more severe conditions like pneumonia or acute diabetic emergencies (DKA/HHS).
Missing Information
- POC glucose, ketones
- CBC, CMP
- Chest imaging
Recommended Plan
Follow evidence-based pathways for URI in T2DM, monitor glucose closely, escalate if deterioration.
Summary
Early Diagnosis
Proactive Patient Care
Homo Habilis 1.0 analyzes patient data from the EHR to identify subtle patterns and risk factors that precede clinical symptoms. It enables clinicians to move from reactive treatment to proactive intervention.
Action: Recommends further investigation based on combined risk factors.

Precision Diagnostics
Homosapieus
At Homosapieus, we provide evidence-based patient diagnosis using our AI-powered platform that integrates with the EHR, enabling doctors to deliver more precise and accurate diagnoses to their patients.The current healthcare landscape is often reactive, with critical patient information siloed within complex Electronic Health Records (EHRs). This system leads to clinician burnout and missed opportunities for early intervention. At Homosapieus, we are fundamentally overhauling this paradigm by embedding intelligent AI directly into medical workflows.
Our AI co-pilot seamlessly integrates with existing EHRs, acting as a vigilant partner for healthcare professionals. It intelligently analyzes vast streams of patient data—from clinical notes and lab results to medical imaging—to identify subtle patterns and risk factors. This dramatically increases diagnostic precision and enables the early detection of diseases long before they become critical.
We are building an ecosystem where AI doesn't just assist, but actively collaborates to create a proactive, data-driven standard of care. Our mission is to empower clinicians with superhuman insights, reduce administrative burdens, and make precision medicine the norm, transforming the health journey with unparalleled accuracy and care.
A Predictive Evidence based Reasoning, Personalised
Health Platform — for People
and Practitioners.
From subtle symptoms to clear predictions. Our AI connects the dots in your health story long before a condition becomes critical.

mg/dL
Blood Glucose
A patient reported feeling unusually tired and thirsty, dismissing it as stress. This elevated glucose level points towards a metabolic imbalance like pre-diabetes.

μIU/mL
Thyroid (TSH)
Subtle but persistent symptoms like sensitivity to cold and hair thinning were logged. This high TSH reading is a strong indicator for hypothyroidism.

ng/mL
Ferritin
A user tracked dizziness and shortness of breath during light exercise. This low ferritin level is a classic sign of iron deficiency, prompting a targeted look at anemia.

bpm
Resting Heart Rate
Through wearable data, the platform detected a rising resting heart rate. This can be an early warning of cardiovascular strain, even if the user feels 'fine'.
mg/dL
Blood Glucose
A patient reported feeling unusually tired and thirsty, dismissing it as stress. This elevated glucose level points towards a metabolic imbalance like pre-diabetes.
μIU/mL
Thyroid (TSH)
Subtle but persistent symptoms like sensitivity to cold and hair thinning were logged. This high TSH reading is a strong indicator for hypothyroidism.
ng/mL
Ferritin
A user tracked dizziness and shortness of breath during light exercise. This low ferritin level is a classic sign of iron deficiency, prompting a targeted look at anemia.
bpm
Resting Heart Rate
Through wearable data, the platform detected a rising resting heart rate. This can be an early warning of cardiovascular strain, even if the user feels 'fine'.
AI agents collaborate
challenge and refine a diagnosis based on a complex patient case demonstrating amulti-perspective approach to clinical reasoning.
Agent Processing Flow
System
Dr Hypothesis Agent
Dr Checklist Agent
Dr Challenger Agent
MAI Dx Orchestrator
Clinical Decision System
Diagnostic Performance Results
Comprehensive analysis of Our pipeline on Undiagnosed diabetes patients
Diabetes Diagnostic
AI Model Comparison
Our comprehensive evaluation reveals that Gemini 2.5 Pro achieves superior diagnostic accuracy at 98%, significantly outperforming other leading AI models. Claude Opus follows at 93%, ChatGPT-4 at 90%, and Deep Seek at 86%. The analysis demonstrates consistent performance advantages across various diabetes-related medical conditions, with particularly strong results in complex diagnostic scenarios. These findings highlight the importance of advanced AI capabilities in clinical decision support systems.
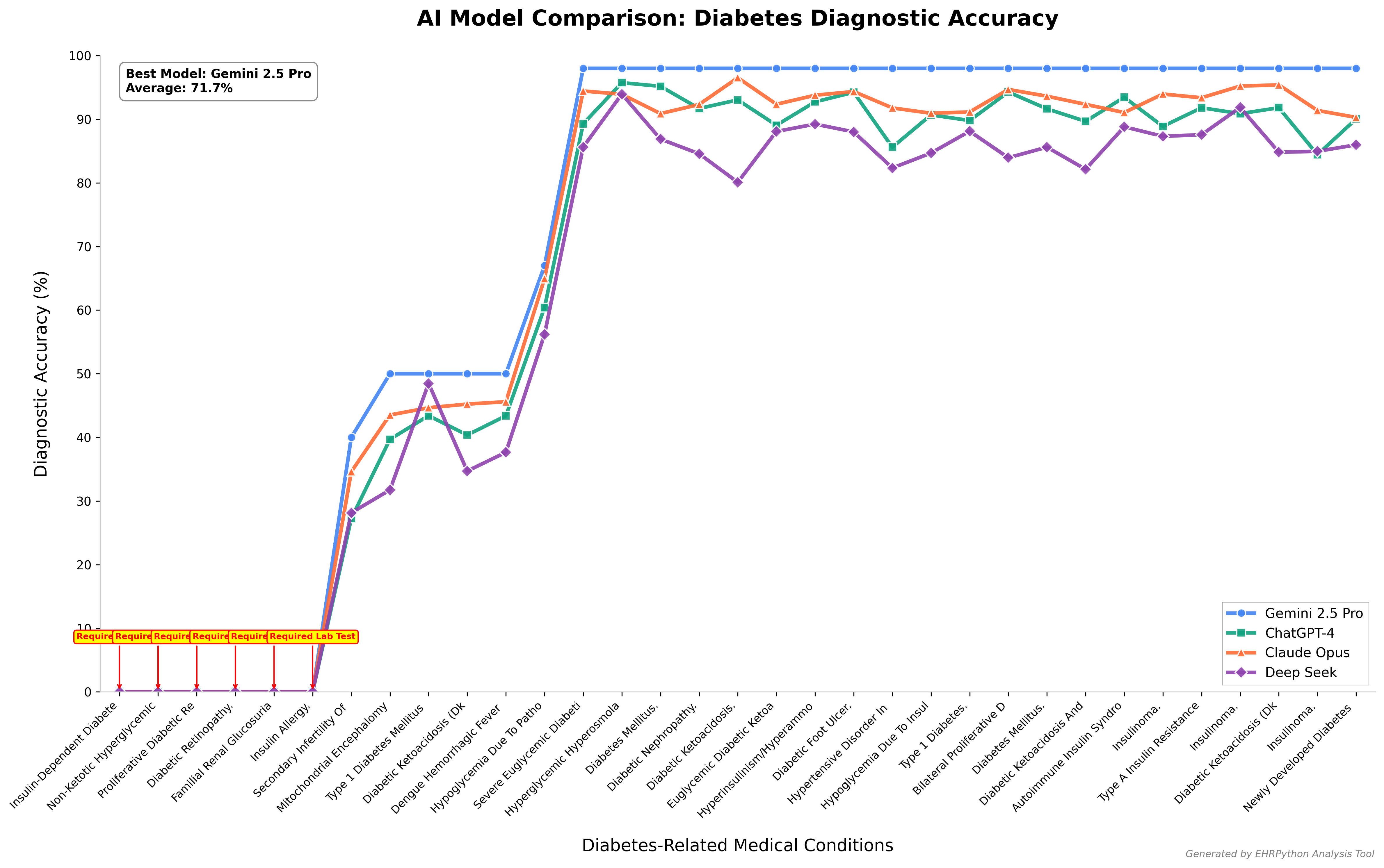
Diabetes Diagnostic Accuracy Across Medical Conditions
* These results are based on controlled testing environments with standardized datasets. Individual performance may vary based on specific use cases, data quality, and implementation factors. All AI diagnostic tools should be used as decision support systems alongside qualified medical professionals.
Clinical Case Analysis
Real-world example of AI diagnostic performance
AI Diagnosis
Primary Assessment
Hypoglycemia secondary to exogenous insulin use, with possible factitious disorder,Type 1 Diabetes Mellitus, and potential HAAF (Hypoglycemia-Associated Autonomic Failure).
Clinical Recommendations
• Confirmed Whipple's triad for hypoglycemia diagnosis
• Immediate endocrinology and psychiatric consultations
• Comprehensive diabetes education and CGM implementation
• Consider insulin pump with threshold suspend feature
• Regular follow-up for psychological support and treatment adherence
Patient Case
25-year-old Iranian Medical InternA 25-year-old Iranian medical intern with T1DM since age 18 (on regular insulin + NPH: Regular 10U breakfast/dinner, 6U lunch; NPH 25U AM, 10U PM) was found unconscious and unresponsive at 3 AM in the doctors' room after their shift. They weigh 57 kg (BMI 20.54 kg/m²) and have a 2-year history of hypoglycemia unawareness, experiencing 3+ severe hypoglycemic episodes weekly over the last 3 months, mostly at night. The patient had been maintaining an active work shift schedule with inadequate eating while maintaining their usual insulin dose, and had recently started a gym exercise routine for glycemic control.Critical findings: BG 25 mg/dl, BP 140/70, HR 110, O2 98%, Temp 36.8°CLabs: High insulin level, low C-peptide level, normal thyroid/kidney/liver functionTreatment: IV 50% dextrose administration led to improved consciousness, with resolution of focal neurological symptoms (hemiparesis, aphasia) within 1 hour.
For Personal Use
For individuals seeking clarity and balance.
Accessible Expert Care
AI-driven insights from your health data without needing a specialist appointment.
Instant Reporting
Upload lab results and get easy-to-understand reports in minutes.
Early Risk Detection
Our AI spots potential health issues long before symptoms become obvious.
Precise Health Insights
See exactly what’s improving in your health and what needs more support.
Proactive Guidance
Know what to do next to prevent health problems from escalating.
Personalised Actionable Plans
Get nutrition, lifestyle, and supplement suggestions tailored to your unique biology.
Dynamic Health Feedback
Your health plan adjusts automatically as your biology and lifestyle evolve.
Secure Health Data
End-to-end encrypted health data that you fully own and control.
For Professional Use
For practitioners delivering truly personalised care.
Comprehensive Screening
Analyze 500+ Rare Disease and over 1,800 subjective inputs in one unified system.
Intelligent Clinical Reporting
Instantly generate functional reports that interpret the full patient health picture.
Automated Health Alerts
Auto-flag emerging patterns and at-risk patients based on real-time data analysis.
Data-Driven Insights
Blend biometrics with clinical notes for personalised, precision-led care.
Predictive Analytics
Anticipate patient dysfunction and disease trends before symptoms arise.
Overall Patient Health Index
A single score summarizing patient vitality, risk, and progress over time.
Probability of Dysfunction
Model what’s likely to develop in a patient — before it does.
Retrospective Heatmaps
Track marker-by-marker change across time, treatments, and protocols.
Scheduled Check-Ins
Automate patient review cadence for improved retention and better results.
AI-Powered Healthcare Solutions
Transform your healthcare practice with advanced AI capabilities. From automated documentation to intelligent workflow management.
What Our Mission Statement
Healthcare systems globally are drowning in preventable diagnostic errors that claim millions of lives annually. Our mission is to revolutionize diagnostic accuracy through AI-powered precision medicine, eliminating the deadly gaps in medical decision-making across India, USA, and beyond.
Americans die or suffer permanent disability from diagnostic errors yearly
of seriously ill hospitalized patients experience diagnostic errors
of diagnostic errors occur during critical testing processes
adults experiences a diagnostic error each year
medical error deaths occur annually in India
of urban healthcare facilities in India have adopted digital health records
of healthcare costs in India are out-of-pocket payments for patients
of digital health implementations in India fail due to data interoperability issues


We Will Detect Diseases Before They Harm You.
Join the waitlist for early access, founding member benefits, and exclusive launch offers.